
Biotech 101: AI Drug Discovery & Precision Medicine
Where are we within the Drug Discovery & Precision Medicine advancement?

AI drug discovery is no longer just about asking, “Can AI design a molecule?”
That was the early hype cycle.
The more important question now is:
Can AI help us choose the right biological target, design the right therapy, test it in the right patients, and improve the odds that a drug actually works?
That is where AI drug discovery and precision medicine start to merge.
Traditional drug development is brutally expensive and slow. A drug can look promising in a lab, survive preclinical testing, enter human trials, and still fail years later because the biology was wrong, the patient group was too broad, or the clinical trial was poorly designed. Recent analysis still shows overall clinical success rates in the low-teens, which means most drug candidates fail somewhere along the journey.
1. The full value chain: AI is moving across the whole drug lifecycle
The easiest way to understand this market is to stop thinking of “AI drug discovery” as one thing.
| Stage | What it means | How AI is used |
|---|---|---|
| 01. Disease biology & target discovery | Understand disease mechanisms and identify promising drug targets. | Genomics & multi-omics analysis; biological network modelling; literature and data mining; target prioritisation. |
| 02. Molecule / protein design | Design and optimise molecules, proteins, antibodies, or biologics that can act on the target. | Generative models for molecules/proteins; structure prediction and optimisation; binding affinity prediction; ADMET and toxicity prediction. |
| 03. Preclinical testing | Evaluate safety, efficacy, and developability before human trials. | In-silico simulations; predictive toxicology; PK/PD modelling; digital biomarkers; experimental design optimisation. |
| 04. Clinical trial design & execution | Plan and run clinical trials more efficiently with the right patients and sites. | Patient stratification; trial site selection; recruitment optimisation; biomarker analysis; outcome prediction. |
| 05. Regulatory submission | Prepare and submit evidence to regulators for approval. | Regulatory intelligence; document generation and summarisation; evidence synthesis; submission optimisation. |
| 06. Manufacturing | Optimise production processes, scale-up, and quality control. | Process modelling; yield prediction; computer vision for quality control; predictive maintenance. |
| 07. Post-market monitoring | Monitor real-world safety, effectiveness, and patient outcomes after launch. | Real-world data analytics; safety signal detection; risk prediction; patient outcome modelling. |
That is why the category is becoming less about “cool molecule generation” and more about end-to-end R&D infrastructure.
2. Precision medicine is the missing half
Precision medicine asks a very simple but powerful question:
Instead of treating all patients with the same disease as one group, can we identify which patients are most likely to respond?
This matters because many diseases are not one disease biologically. Cancer, Alzheimer’s, ALS, autoimmune diseases, and rare diseases can look similar clinically but have very different underlying biology.
That is where biomarkers, genomics, transcriptomics, proteomics, imaging, blood tests, and companion diagnostics come in. The FDA already maintains a list of cleared or approved companion diagnostic devices, showing that precision medicine is not just a futuristic concept — it is already part of regulated medicine.
The strongest AI companies in this space are not just trying to design drugs faster. They are trying to answer two questions together:
What should we target?
And which patients should receive it?

That second question is why companies like Verge Labs are interesting. Their pitch is not only “AI-discovered drugs,” but disease models that can help predict patient biology — for example, a “virtual biopsy” of the brain from a blood draw.
3. How developed is the sector today?
The sector is promising, but uneven.
Some parts are already quite mature. AI is widely useful for structure prediction, virtual screening, image analysis, ADMET prediction, trial recruitment, site selection, documentation support, and pharmacovigilance. Regulators are also paying serious attention: the FDA issued draft guidance in 2025 on using AI to support regulatory decision-making for drugs and biologics, while the EMA has also published work on AI across the medicinal product lifecycle.
But the hardest part is still not fully proven: AI has not yet consistently shown that it can create better drugs all the way to approval at scale.
That distinction matters.
AI is already improving workflows. It may shorten discovery cycles, improve trial recruitment, and help researchers make better decisions. But “AI-designed drug reaches approval and proves the whole model works” is still the milestone everyone is watching.
4. The newest technologies: foundation models for biology
The most exciting shift is the rise of biology foundation models.
In normal AI, foundation models are trained on large amounts of text, images, code, or multimodal data. In biotech, foundation models are trained on biological data: protein sequences, DNA, RNA, cell states, pathology images, chemical structures, and clinical data.

Examples include:
Protein models that understand protein sequences and structures.
Chemistry models that generate or optimise molecules.
Pathology foundation models that read tissue slides.
Single-cell models that learn how cells behave.
Multimodal disease models that combine omics, imaging, and clinical data.
Closed-loop labs where AI suggests experiments, robots run them, and the results feed back into the model.
AlphaFold was the major psychological turning point because it showed that AI could solve a real biological prediction problem at extraordinary scale. The next wave is moving from “predict structure” to “design interactions, predict biology, and improve therapeutic outcomes.”
That is why Biohub’s protein biology world model and Verge Labs’ disease biology world model are exciting: both are trying to move AI from language or static prediction into biological reasoning.
5. Who is building this?
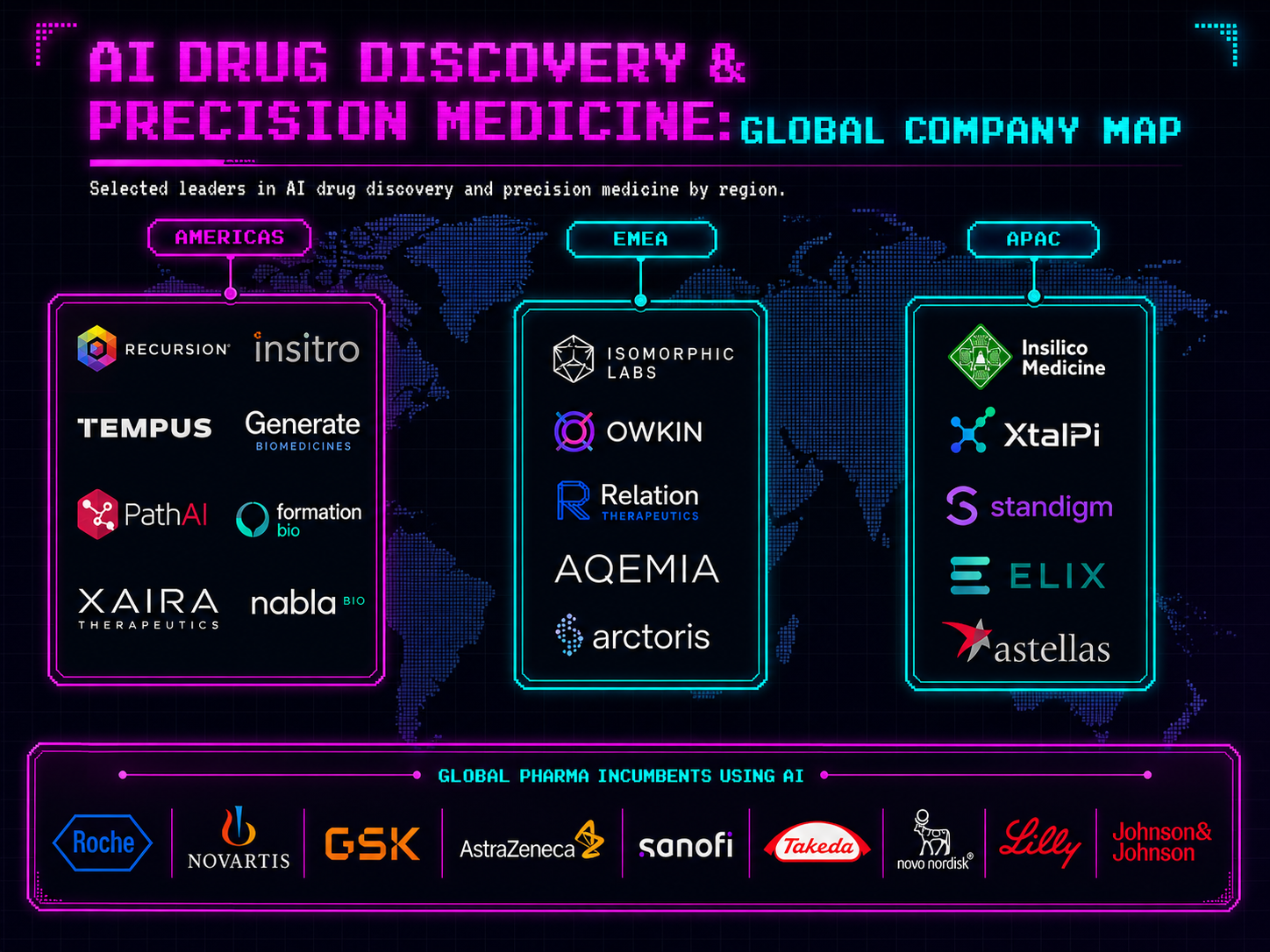
In the US, the market is deep and capital-heavy. Companies like Recursion, insitro, Tempus, Generate Biomedicines, PathAI, Formation Bio, Xaira Therapeutics, and Nabla Bio are building across phenomics, patient data, generative biology, digital pathology, AI-native clinical development, and protein design.
In Europe, the standout names include Isomorphic Labs in London, Owkin in Paris, Relation Therapeutics in London, AQEMIA in Paris, and Arctoris in Oxford. Isomorphic Labs is especially important because it sits close to Google DeepMind and AlphaFold; Reuters reported it raised $2.1 billion in 2026 to scale AI-driven drug discovery.
In APAC, important names include Insilico Medicine, XtalPi, Standigm, Elix, and AI-driven initiatives inside large pharma groups such as Astellas. APAC is particularly interesting because China, Hong Kong, Japan, and Korea are building strength in AI chemistry, automation, simulation, and cross-border pharma partnerships.
Big pharma is also not sitting still. Roche, Novartis, GSK, AstraZeneca, Sanofi, Takeda, Novo Nordisk, Lilly, and J&J are all either partnering with AI biotechs, acquiring AI platforms, or building internal AI infrastructure.
6. The business model is not just SaaS
This is not a clean software market.
AI biotech companies can make money in several ways:
They can sell software or platform access.
They can partner with pharma for milestone payments.
They can build internal drug pipelines.
They can own proprietary datasets.
They can run automated labs.
They can develop companion diagnostics.
They can support clinical trials and regulatory workflows.
The strongest companies often mix several of these models.
Pure software is attractive because margins can be high, but pharma value usually compounds around assets, data, and clinical proof. That is why many AI drug discovery startups are not trying to be “the Salesforce of biotech.” They are trying to become a new kind of AI-native pharma infrastructure company.
7. Why investors care
The opportunity is huge because pharma R&D is huge, slow, and inefficient. Even a small improvement in success rates, trial speed, or patient selection could create massive value.
That is also why funding rounds in this sector can look insane. Xaira launched with over $1 billion in committed funding. Formation Bio raised hundreds of millions. Isomorphic has raised billions. These are not lightweight app startups; they need compute, data, labs, scientists, clinical operations, and regulatory expertise.
The investor thesis is basically:
If AI can reduce even a small part of drug development failure, the value pool is enormous.
8. The challenges are still very real
The biggest challenge is data. Biology data is messy, fragmented, expensive, private, and often not comparable across labs or hospitals. Unlike internet text, high-quality biomedical data is not freely sitting everywhere waiting to be scraped.
The second challenge is validation. A model can perform well on benchmarks and still fail in the real world. Biology is annoying like that. Cells do not care about your pitch deck.
The third challenge is regulation. AI used in drug development needs traceability, context-of-use validation, and evidence that the model is reliable for the specific decision it supports. That is exactly why FDA and EMA guidance matters.
The fourth challenge is adoption. Doctors, researchers, regulators, and pharma teams need to trust the output. In healthcare, “the model said so” is not enough.
And the fifth challenge is capital intensity. The best companies need not only AI talent, but also wet labs, clinical data, biology expertise, regulatory infrastructure, and sometimes manufacturing knowledge.
9. What happens next?
My view: the next decade will not be “AI replaces pharma scientists.”
It will be:
AI becomes the operating system of drug development.
The near-term wins will come from better target prioritisation, faster screening, better trial recruitment, richer biomarker strategies, and more efficient regulatory and clinical workflows.
The bigger, harder win will be proving that AI can consistently improve the probability of clinical success. That is the holy grail.
The companies I would watch are the ones that connect three things:
Proprietary biological data
Closed-loop experimental validation
Patient stratification / precision medicine
Because the future is not just designing a drug faster. It is designing the right drug, for the right biology, in the right patient group.

